






























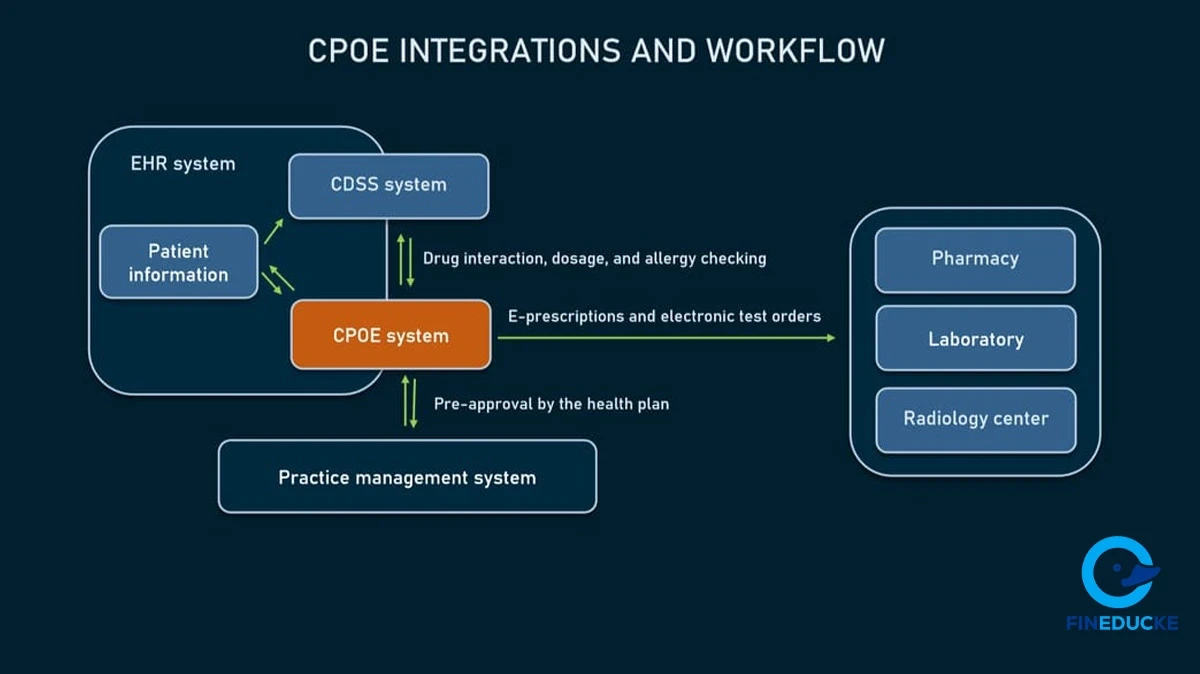
The adoption of health information technology is an incredibly complicated sociotechnical concern, and it has long since gone beyond mere software installation and into the very essence of clinical culture and practice. Following the study of the effectiveness of Computerized Provider Order Entry (CPOE) technology in reducing medication mistakes, Poon et al. (2004) found that most organizational and human challenges acted as barriers to its implementation in many organizations.
These real-life barriers are described in detail by Katz et al. (2010) in their case study of the CPOE implementation at Emory Healthcare. A detailed discussion of this example makes it possible to deconstruct the particular concerns of executive management, healthcare professionals, and support staff. This analysis evaluates three major implementation issues: important workflow failures, the introduction of a faulty system module, and ineffective change management, and provides project management solutions that may have supported a more successful changeover.

The CPOE project's strategic drive was fuelled by the explicit goals of the Emory administration. Katz et al. (2010) explain how the Chief Quality Officer, Dr. Bill Bornstein, perceived the system as a major tool in clinical care standardization. His key goal was to decrease the inconsistency in treatment, which he regarded as the immediate cause of medical errors and risks associated with patient safety.
The executive vision was process improvement, which identified technology as having the ability to impose best practices and reduce the complexity clinicians had to deal with.
A sense of reality had, however, put a check on this strategic vision on the inadequacy of the technology. Dr. Bornstein was not afraid to acknowledge the general immaturity of the CPOE system and the serious flaws of the specific aspects, such as the medication reconciliation module (Katz et al., 2010).
The problem that they were forced to face was that they were trying to pursue the strategic goal of standardization, whilst they were obliged to face the fact of operations of having a system with known weaknesses in it; that being a trade-off, as well as the after-effects of implementation.
The CPOE system was a profound change in workflow and professional independence for the clinical practitioners, as it generated a spectrum of responses, including the reluctance to embrace the change and the unwillingness to do so. Katz et al. (2010) articulate the entrenched mistrust of a doctor like a neurosurgeon, Dr. Jeff Olson, who thought that the standardized order sets were too rigid to respond to specific and complicated care that his targeted patients required.
This may be associated with the overall outcomes, which CPOE would introduce a predetermined and unnatural connection between clinical activities and disrupt the standard practice patterns (Niazkhani et al., 2009). This system was viewed not as an instrument of assistance to clinical practices but rather as an obtrusive administrative unit that made the basic process of patient care more complex.
Besides the philosophical arguments, the physicians were facing practical and more immediate barriers to usability that led to new avenues of error. The new system, as viewed by one of the emergency doctors, Dr. Andre Matthews, featured some strong points, including customizability, but had more pitfalls, like the entry of the order of the wrong patient because of an incorrectly located mouse click (Katz et al., 2010).
These issues are instances of CPOE systems, which generate or uncover a deep level of problems in human-computer interactions, fundamentally changing the interactions and the tempo of the clinical work (Campbell et al., 2009). The technology itself was a consequence of the constant vigilance that physicians required in order to avoid mistakes created by the systems.
Such an application meant that there was a radical difference in impacts between subordinate and support staff, which practically re-established the distribution of labor. The CPOE system left a significant impression on the workflow among the nursing staff members, who felt that it had introduced a communication gap. According to Katz et al. (2010), Anna Bonner, a floor nurse, noted that the unit clerk was a man who was known as a gatekeeper and was in charge of the information flow in the unit and the notification of employees about the urgent tasks.
This banishment of an essential middleman coincides with research findings indicating that CPOE systems do not generally support all clinical workers fully, contributing to workload disparities and requiring nurses to be more proactive in finding information in less predictable situations (Campbell et al., 2009). Accordingly, the CPOE system changed the role of the nurse as a coordinator of care delivery to a troubleshooter of a disjointed digital process in some cases.
Conversely, the overall job role of pharmacists changed significantly in a positive way. According to Katz et al. (2010), pharmacist Tony Ottaviano stated that CPOE has relieved pharmacists of the time-consuming process of entering medication orders manually.
This redistribution of labor enables the pharmacists to transition off the pharmacy into more of an active clinical role on the hospital floors, where they can directly participate in the enhancement of medication safety at the point of care.
One of the biggest downsides to the Emory case was the crucial failure of the workflow that should have been predicted and prevented, particularly regarding high-risk patient handoff. One example is the transference of patients after the anesthesia stage between the Post-Anesthesia Care Unit (PACU) and the hospital floor. Katz et al. (2010) explain that the CPOE system was a poorly fitted logic of initiating orders, which disrupted a prior efficient, informal process. Patients were still physically in the PACU but were receiving floor orders, causing confusion, lab draws to be missed, and imaging studies to be left incomplete.
High-fidelity process simulation was not the focal point of the approach; rather, it focused on generic classroom training. The project manager should have required interdepartmental teams to enact a thorough and detailed scenario-based walkthrough of the whole patient transfer process via the CPOE test environment; teams that should have included surgeons, anesthesiologists, PACU, and floor nurses.
A culture of active assistance, as advocated in an effective implementation, is essential to identify the presence of such hidden lapses in the processes (Gellert et al., 2015). This would have required the team to either come up with technical solutions or create an unambiguously understood universal manual workarounds for unpredictable scenarios.
The second significant obstacle was that the team decided to implement one of the central system elements, the medication reconciliation module, which was considered to have a very grave flaw. The module was counterintuitive and redundant to the extent that physicians saw it as a significant obstacle (Katz et al., 2010). This poor usability also resulted in the project director being eventually compelled to switch off the module after the adoption, which is a testament to the failure of the pre-deployment validation step.
A more stringent User Acceptance Testing (UAT) program dedicated to the high-risk clinical functions would have helped to avoid this issue. Given that studies validate that even minor design issues impact physician adoption and error reduction (Khajouei & Jaspers, 2010), a project manager should have empowered a special testing group of clinical skeptics to formally test the module against real-life situations.
According to Khajouei and Jaspers (2010), such reviews need to ensure that the interface is cognitively simple to perceive and has a natural sequence of clinical operations. This process would have generated the hard evidence needed to either demand a vendor redesign or make the strategic decision not to deploy the faulty feature from the beginning.
The Emory implementation was plagued by a poor change management strategy whose implementation was more based on coercion rather than cooperation to achieve a goal, resulting in alienation of physicians. The leadership admitted to intimidating physicians with attempts to force them to accept the standardized order sets even in the event that they did not correspond with the consensus (Katz et al., 2010).
This was a grave threat to the future rollout opportunities, especially at centers like Emory University Hospital Midtown that had a large number of independent community physicians who were not as much of an administrative part of the facility.
An enhanced project management strategy would have been geared towards participative governance and precise integration. Gellert et al. (2015) point to the establishment of a clinical IT steering committee with executive and physician leadership as a key factor in their success. According to this model, resistance could have been minimized by the project manager through the development of physician-led, specialty-based workgroups to design and test the order sets.
A customer-oriented approach to health IT change is an important aspect of change management as the clients are the key partners whose needs must be satisfied (Gellert et al., 2015). This proactive and as wide as possible approach changes the process of implementation from more of a mandate in a top-down approach to making institutional commitments.
The change to CPOE in Emory Healthcare is an apt illustration that the feasibility of substantial health IT construction does not necessarily lie in technology but in the organization's management ability to respond to people and process implications of the adoption. Challenges such as dislocation of the workflow, insufficient system usability, and deficient change management were not, quite literally, technical problems, but the results of a lapse of foresight, validation, and coordination.
Emory’s experience left no doubt that to cope with such barriers, it was an extreme necessity to be immersed in the study of the needs of all parties involved, pursue the thorough testing of the practical scenarios being considered, and be wholly responsive to a change management approach that leads to the development of trust. These are the components that would bridge the gap between the hypothetical benefits of a healthcare IT system and its real-life application and successful implementation in a problematic clinical environment.
Katz, A., LaBorde, D., McFarlan, F. W., Keil, M., Morgan, M., & Hamermesh, R. G. (2010). Computerized provider order entry at Emory Healthcare. Harvard Business School Cases, 1.
Campbell, E. M., Guappone, K. P., Sittig, D. F., Dykstra, R. H., & Ash, J. S. (2009). Computerized provider order entry adoption: Implications for clinical workflow. Journal of General Internal Medicine, 24(1), 21–26.
Gellert, G. A., Hill, V., Bruner, K., Maciaz, G., Saucedo, L., Catzoela, L., Ramirez, R., Jacobs, W. J., Nguyen, P., Patel, L., & Webster, S. L. (2015). Successful implementation of clinical information technology: Seven key lessons from CPOE. Applied Clinical Informatics, 6(4), 698–715.
Khajouei, R., & Jaspers, M. W. M. (2010). The impact of CPOE medication systems' design aspects on usability, workflow, and medication orders: A systematic review. Methods of Information in Medicine, 49(1), 3–19.
Niazkhani, Z., Pirnejad, H., Berg, M., & Aarts, J. (2009). The impact of computerized provider order entry systems on inpatient clinical workflow: A literature review. Journal of the American Medical Informatics Association, 16(4), 539–549.
Poon, E. G., Blumenthal, D., Jaggi, T., Honour, M. M., Bates, D. W., & Kaushal, R. (2004). Overcoming barriers to adopting and implementing computerized physician order entry systems in U.S. hospitals. Health Affairs, 23(4), 184–190.
The Fineducke Team is a group of passionate writers, researchers, & finance enthusiasts dedicated to helping the youth make smarter money decisions. From saving tips, investment ideas to digital income guides, our team works together to bring you easy-to-understand, practical content tailored for everyday life believing financial education should be simple & relatable.












































Leave a Comment:
Please log in to leave a comment.
Comments:
No comments yet. Be the first to comment!